Printable Dental Claim Form
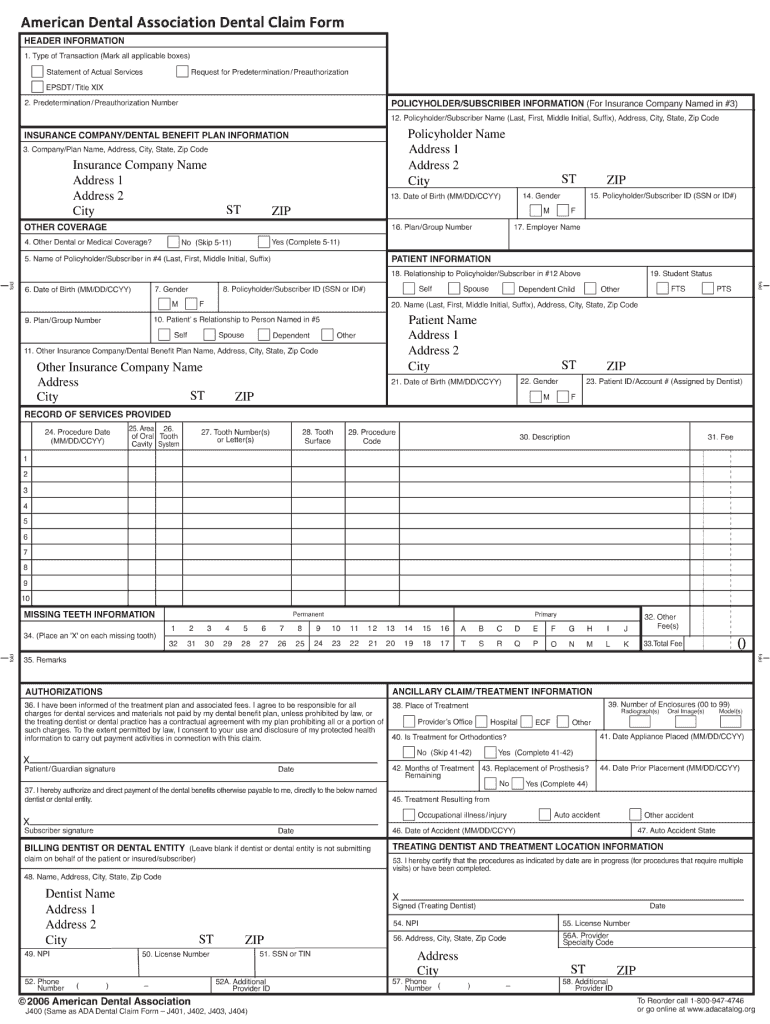
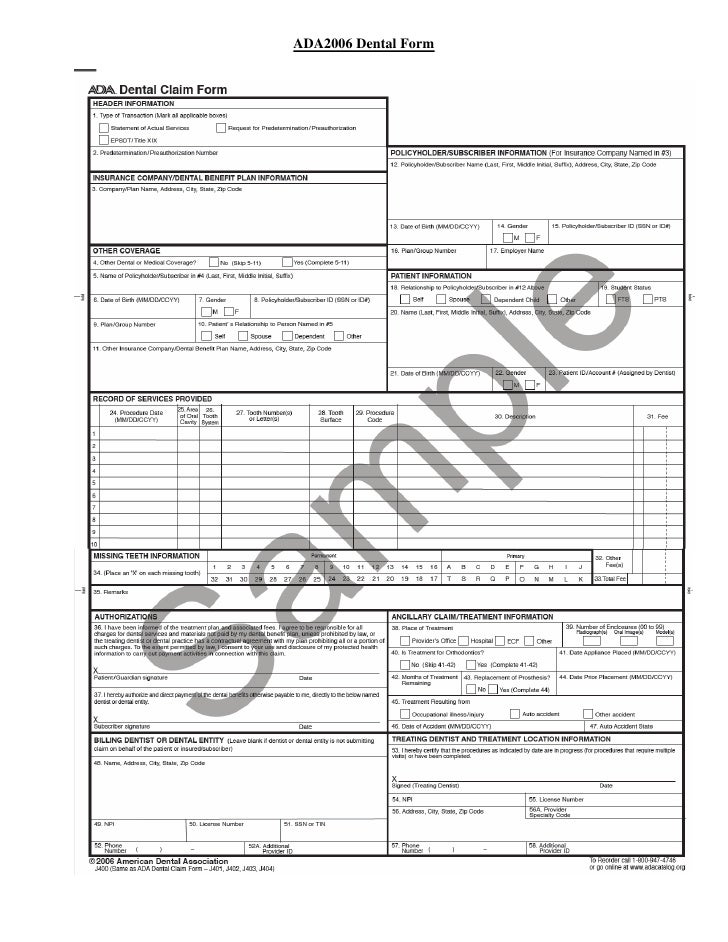
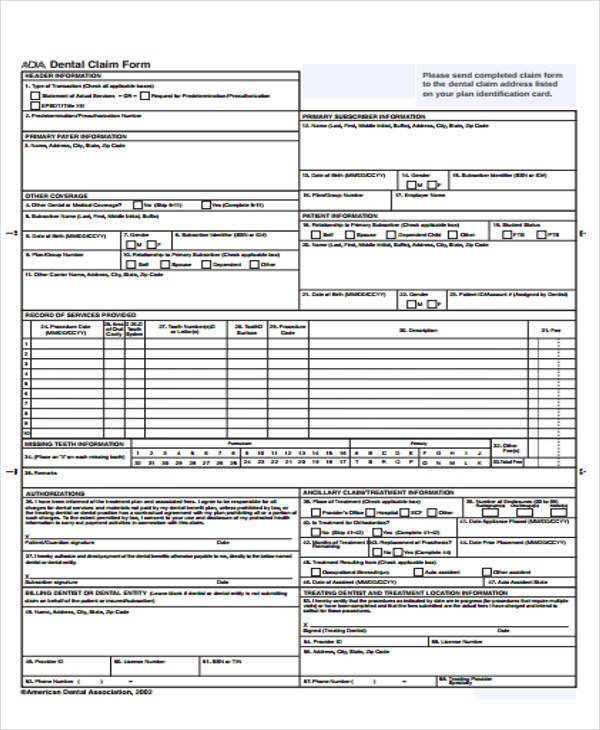
Printable Dental Claim Form - Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. Web this version of the ada form incorporates editorial changes to further its consistency with the 837d. Humana doesn't require a specific dental claim form. Patient’s name (first, middle initial, last) 4. Date of birth (mm/dd/ccyy) 14. Web dental claim form type of transaction (mark all applicable boxes) request for predetermination/preauthorization statement of actual services epsdt/title xix. Get the answers you need here! Tooth number(s) cavity system or letter(s) 28. (mm/dd/ccyy) of oral tooth 27. Other fee(s) 1 2 3 4 5 6 7. (mm/dd/ccyy) of oral tooth 27. Web submit the typed claim form directly to aflac at: Please download your copy of the ada 2019 claim form and start using this. Tooth number(s) cavity system or letter(s) 28. Web dental claim form type of transaction (mark all applicable boxes) statement of actual services request for predetermination/preauthorization epsdt/title xix. Web claim forms that are submitted with missing or misplaced information can slow or even stop our ability to. Your dentist will submit your dental claim directly to humana. Web for information about licensing of the ada dental claim form, please see cdt. Incomplete claim forms will be returned to you for missing information. Ad search for answers from across. Web submit the typed claim form directly to aflac at: Your dentist will submit your dental claim directly to humana. To begin with, find the “get form” button and press it. Incomplete claim forms will be returned to you for missing information. Date of birth (mm/dd/ccyy) 14. Please download your copy of the ada 2019 claim form and start using this. For any questions regarding pricing or purchasing copies of the ada dental claim form,. Group number or enrollment code 3. Signnow allows users to edit, sign, fill and share all type of documents online. Tooth number(s) cavity system or letter(s) 28. Web of this form.) s dental claim form please type or print 1. Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. Web claim forms that are submitted with missing or misplaced information can slow or even stop our ability to. Web the american dental association (ada) offers a comprehensive health history form, for adults or. Other fee(s) 1 2 3 4 5 6 7. Web submit the typed claim form directly to aflac at: (mm/dd/ccyy) of oral tooth 27. Ad download or email ada j430 & more fillable forms, register and subscribe now! Web dental claim form type of transaction (mark all applicable boxes) statement of actual services request for predetermination/preauthorization epsdt/title xix. Other fee(s) 1 2 3 4 5 6 7. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into. Please download your copy of the ada 2019 claim form and start using this. Missing teeth information (place an “x” on each missing. Web read the following instructions to use cocodoc to start editing and finalizing your printable dental claim form: Edit, sign and save ada dental claim form. Tooth number(s) cavity system or letter(s) 28. Incomplete claim forms will be returned to you for missing information. For any questions regarding pricing or purchasing copies of the ada dental claim form,. Web submit the typed claim form directly to aflac at: Your dentist will submit your dental claim directly to humana. Please correct these common issues before submitting the claim to delta. Web this version of the ada form incorporates editorial changes to further its consistency with the 837d. Humana doesn't require a specific dental claim form. Tooth number(s) cavity system or letter(s) 28. Ad search for answers from across the web with superdealsearch.com now. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into. Incomplete claim forms will be returned to you for missing information. Ad download or. Edit, sign and save ada dental claim form. (mm/dd/ccyy) of oral tooth 27. Please download your copy of the ada 2019 claim form and start using this. Web dental benefits claim form. To begin with, find the “get form” button and press it. Group number or enrollment code 3. Web 1 2 3 4 5 6 7 8 9 10 33. Web medicare advantage dental claim forms. Web dental claim form type of transaction (mark all applicable boxes) statement of actual services request for predetermination/preauthorization epsdt/title xix. For any questions regarding pricing or purchasing copies of the ada dental claim form,. Patient’s name (first, middle initial, last) 4. Ad search for answers from across the web with superdealsearch.com now. You can complete and submit this form, or your dental provider can submit a claim on your behalf. Signnow allows users to edit, sign, fill and share all type of documents online. Web this version of the ada form incorporates editorial changes to further its consistency with the 837d. Policyholder/subscriber name (last, first, middle initial, sufix), address, city, state, zip code 13. (mm/dd/ccyy) of oral tooth 27. Web the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code reporting that was also incorporated into. Web of this form.) s dental claim form please type or print 1. Web print find a form applications and forms for dentists and their patients claims disputes and appeals era/eft national provider identifier network application salzmann.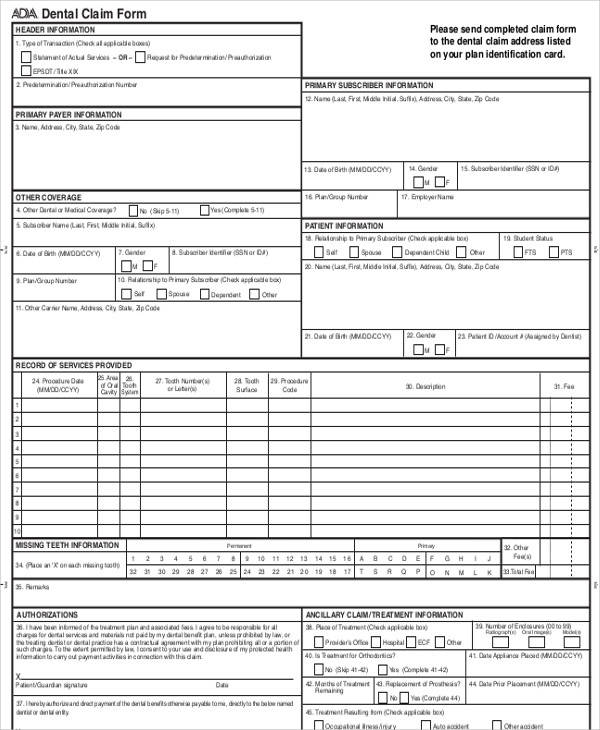
FREE 47+ Claim Forms in PDF

Physicians Mutual Insurance Company Dental Insurance Claim Form. Dental
Printable Dental Claim Form 2018 Fill and Sign Printable Template

Free Printable Ada Dental Claim Form Printable Templates
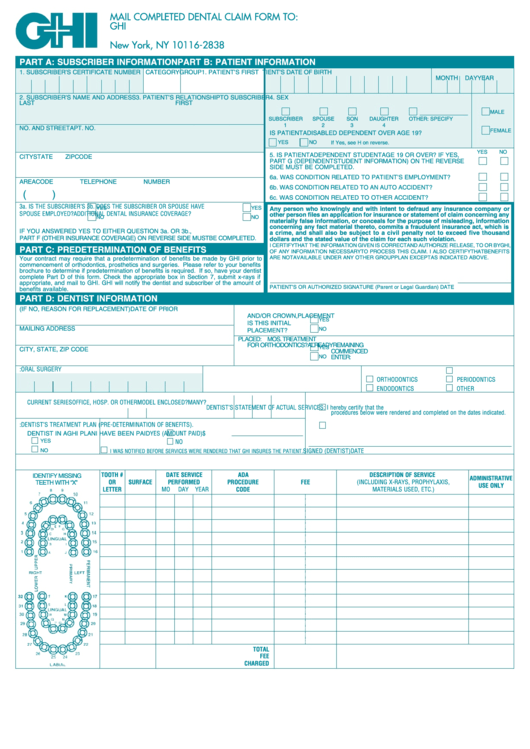
Form D437b Ghi Dental Claim Form printable pdf download
Free Printable Ada Dental Claim Form
Printable Dental Claim Form
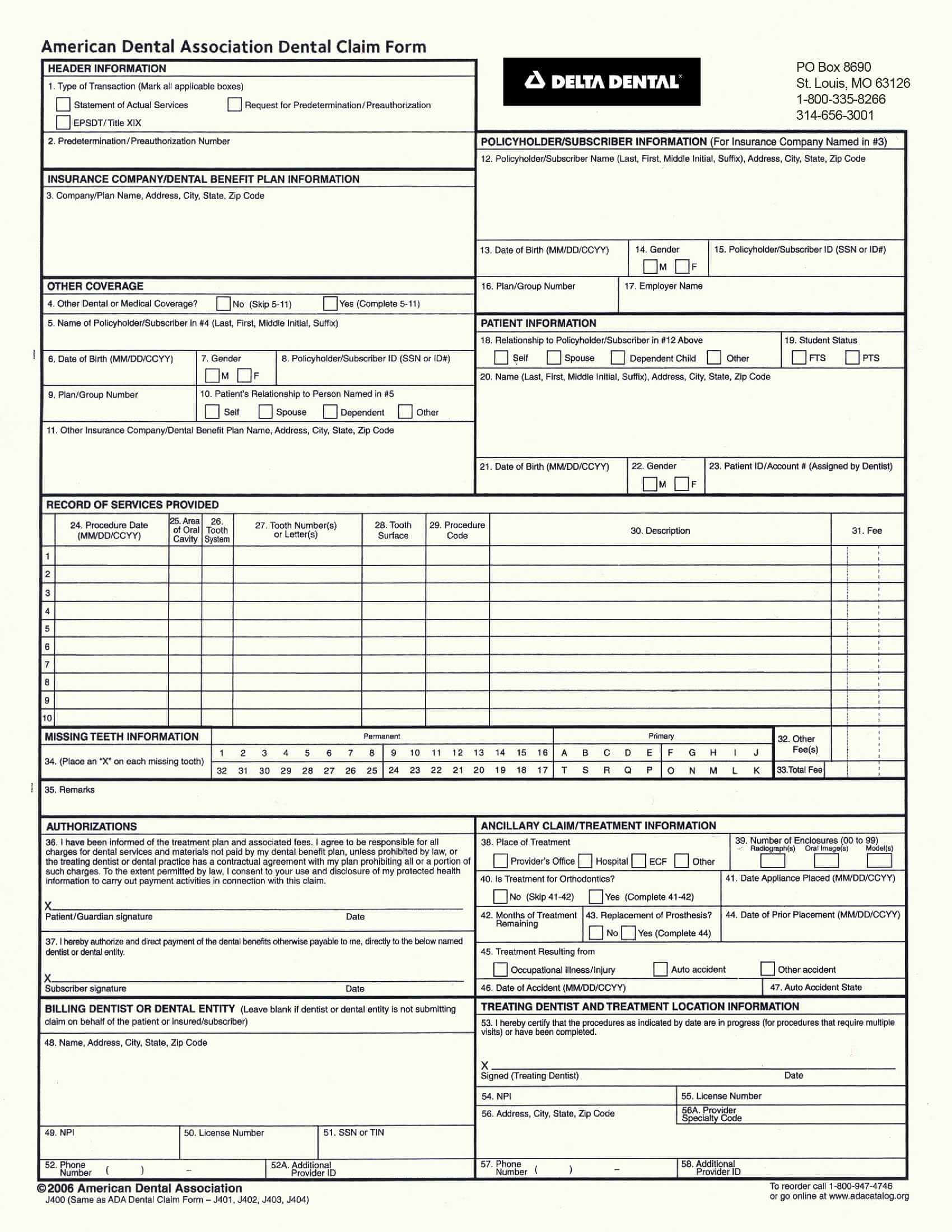
Delta Dental Claim Form
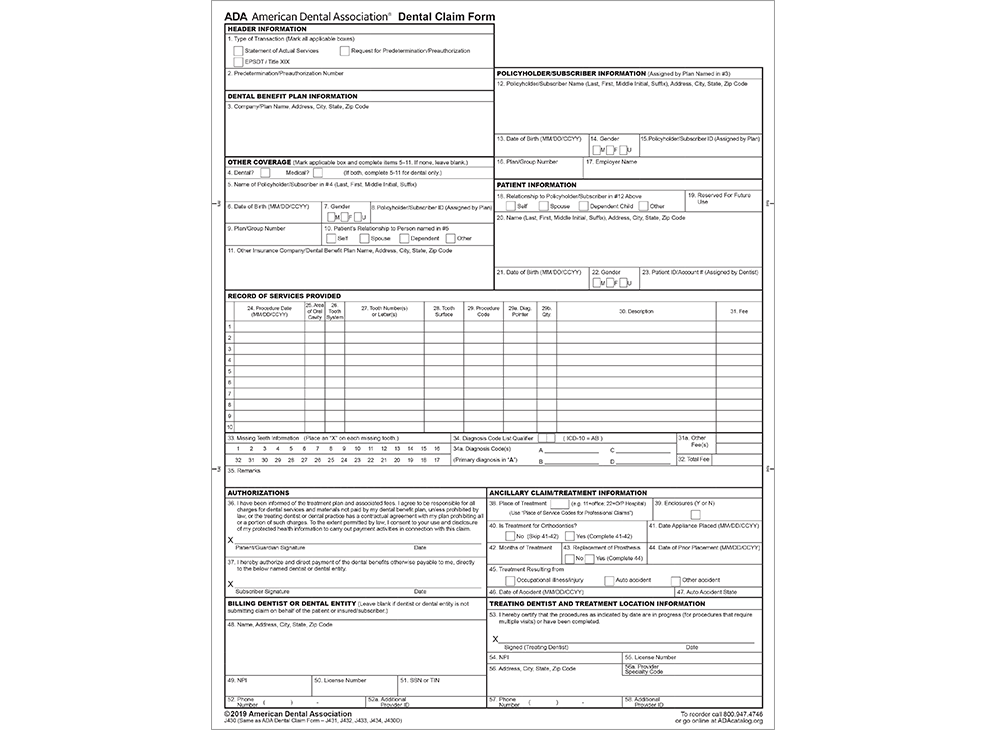
ADA Store Dental Claim Form (2019 Version) Downloadable PDF

Dental Claim Form Fill and Sign Printable Template Online US
Related Post: